I'm beginning, for this blog, a series of short utility scripts and essays that relate, in one way or another, to the general subject of indexing and data retrieval.
The first entry is a short Perl script (just 18 command lines) that extracts the names (of people) wherever the names may occur within a provided text file. The output consists of an alphabetized list of non-repeating names. The script is so simple that it can be easily be translated into any language that supports regular expressions (regex).
The script is available at:
http://www.julesberman.info/factoids/namesget.htm
Blog readers who are uninterested in indexing and data retrieval may want to visit my two other blogs,
Machiavelli's Laboratory (scientific ethics taught from the perspective on an unethical scientist)
and
Neoplasms (essays on tumor biology)
- © 2010 Jules Berman
key words: indices, indexing, indexes, index, data retrieval, information retrieval, informatics
Wednesday, October 27, 2010
Thursday, October 14, 2010
Germ cell tumor web page available
The recent blog series on germ cell tumors has been packaged into a single web page available at:
http://www.julesberman.info/factoids/germcell.htm
- © 2010 Jules Berman
key words: carcinogenesis, neoplasia, neoplasms, tumor development, tumour development, tumor biology, tumour biology, carcinogenesis
http://www.julesberman.info/factoids/germcell.htm
- © 2010 Jules Berman
key words: carcinogenesis, neoplasia, neoplasms, tumor development, tumour development, tumor biology, tumour biology, carcinogenesis
Monday, October 11, 2010
New blog site on Neoplasms
Readers who are primarily interested in medical informatics may have found the past week's blogs on germ cell tumors to be a bit off-track. I agree. I've created a new blog site, Neoplasms, to cover my interests in tumor biology.
Henceforth, for the Specified Life blog, I'll stick to issues of data retrieval, organization, indexing, annotation, and analysis.
For readers who have been following the germ cell series, you might be interested in a new blog series I'll be starting, on "epigenomic tumors", in the Neoplasms blog site. I'll be starting with a discussion of malignant rhabdoid tumors.
- © 2010 Jules Berman
key words: carcinogenesis, neoplasia, neoplasms, tumor development, tumour development, tumor biology, tumour biology, carcinogenesis
Henceforth, for the Specified Life blog, I'll stick to issues of data retrieval, organization, indexing, annotation, and analysis.
For readers who have been following the germ cell series, you might be interested in a new blog series I'll be starting, on "epigenomic tumors", in the Neoplasms blog site. I'll be starting with a discussion of malignant rhabdoid tumors.
- © 2010 Jules Berman
key words: carcinogenesis, neoplasia, neoplasms, tumor development, tumour development, tumor biology, tumour biology, carcinogenesis
Thursday, October 7, 2010
Germ cell cancers of testes: conclusion
This is the last entry on a series of blogs on germ cell cancers of the testes.
I've added forward and backward links for each of the blogs in the series, so you can visit the first blog in the series and click forward or backward through the sequential entries.
Basically, in this series, we showed, using the SEER public use data files, that there has been a large increase in the incidence of germ cell cancers of the testis in white non-Hispanic males since the first SEER observation year (1973) up to the most recent data year (2007).
Along with the increase in seminomatous germ cell cancers was a lesser but parallel increase in the non-seminomatous germ cell cancers of the testis, when compared in birth cohort populations.
The seminomatous and non-seminomatous germ cell cancers, though derived from very different cell types (germ cells versus embryonic/extra-embryonic primitive cells) develop from the same precanceous lesion (usually intratubular germ cell neoplasia and sometimes gonadoblastoma). Precancerous germ cells are characterized by epigenomic erasure, and this "erased" state seems to allow precancerous germ cells to develop into seminomas or into tumors derived from totipotent stem cells.
Testicular precancers develop from disorders of sex development. The incidence of disorders of sex development, like the incidence of testicular germ cell cancers, has been rising. The cause for the rise of disorders of sex development (and the concomitant rise in testicular germ cell cancers) is unknown. However, the ubiquitous appearance of the platicizer and endocrine disruptor, Bisphenol A, has captured the interest of toxicologists and cancer researchers.
All of these issues were discussed in this completed series of blogs on testicular germ cell cancers.
- © 2010 Jules Berman
key words: carcinogenesis, neoplasia, neoplasms, tumor development, tumour development, germ cell tumor, germ cell tumour, tumor epidemiology, increasing germ cell cancer rates, germ cell cancer, seminomas, seminomatous, non-seminomatous, non-germinomatous, embryonal carcinoma, choriocarcinoma, testis, testes, itgcn, intratubular germ cell neoplasm, plasticizers, endocrine disruptors
I've added forward and backward links for each of the blogs in the series, so you can visit the first blog in the series and click forward or backward through the sequential entries.
Basically, in this series, we showed, using the SEER public use data files, that there has been a large increase in the incidence of germ cell cancers of the testis in white non-Hispanic males since the first SEER observation year (1973) up to the most recent data year (2007).
Along with the increase in seminomatous germ cell cancers was a lesser but parallel increase in the non-seminomatous germ cell cancers of the testis, when compared in birth cohort populations.
The seminomatous and non-seminomatous germ cell cancers, though derived from very different cell types (germ cells versus embryonic/extra-embryonic primitive cells) develop from the same precanceous lesion (usually intratubular germ cell neoplasia and sometimes gonadoblastoma). Precancerous germ cells are characterized by epigenomic erasure, and this "erased" state seems to allow precancerous germ cells to develop into seminomas or into tumors derived from totipotent stem cells.
Testicular precancers develop from disorders of sex development. The incidence of disorders of sex development, like the incidence of testicular germ cell cancers, has been rising. The cause for the rise of disorders of sex development (and the concomitant rise in testicular germ cell cancers) is unknown. However, the ubiquitous appearance of the platicizer and endocrine disruptor, Bisphenol A, has captured the interest of toxicologists and cancer researchers.
All of these issues were discussed in this completed series of blogs on testicular germ cell cancers.
- © 2010 Jules Berman
key words: carcinogenesis, neoplasia, neoplasms, tumor development, tumour development, germ cell tumor, germ cell tumour, tumor epidemiology, increasing germ cell cancer rates, germ cell cancer, seminomas, seminomatous, non-seminomatous, non-germinomatous, embryonal carcinoma, choriocarcinoma, testis, testes, itgcn, intratubular germ cell neoplasm, plasticizers, endocrine disruptors
Wednesday, October 6, 2010
Explaining the rise in testicular germ cell tumors
In yesterday's blog we saw that the rise in testicular cancer rates in white males showed a parallel increase in seminomatous and non-seminomatous germ cell cancers among birth cohorts.
What can explain this increase?
There is one class of conditions that is overwhelmingly associated with the development of germ cell tumors of the testis: disorders of sex development of the testes.[1] Among the conditions within this general group are testicular dysgenesis, testicular feminization (insensitivity to androgens), and cryptorchidism. Disorders of sex development of the testis raise the incidence of intratubular germ cell neoplasia or of gonadoblastoma, both of which are testicular precancers.
As you might expect, along with the observed increase in testicular germ cell cancers in white males, there has been an observed increase in the incidence of disorders of sex development in the same population. [1,2] These disorders are characterized by a retardation in the maturation of primordial germ cells, along with an apparent mitotic over-stimulation of these same cells: leading to a proliferative, precancerous condition.
Though there is no proof at the moment, we might expect that males who develop testicular germ cell cancer who have clinically normal testes, may harbor small foci of [clinically unobserved] germ cell proliferative lesions.
What has caused the increased incidence of disorders of sex development in the testes? We don't know, but we have a candidate: the ubiquitous plasticizer and endocrine disruptor, Bisphenol A.
Bisphenol A is a synthetic estrogen used in the process of manufacturing plastics, and has been detected in the serum, milk, saliva, urine, and amniotic fluid of humans.[3] Because we get our daily dose of Bisphenol A from plastic bottles, one would expect that the levels of Bisphenol A in our blood would have increased steadily over the past several decades [coinciding with our increased dependence of plastic food and drink containers]. You might also expect that if Bisphenol A produced testicular cancers, you would see the largest increases in incidence among the wealthiest populations in the most industrialized nations [as we do].
Can we assume that Bisphenol A is causing the rise of incidence of testicular germ cell cancers? Absolutely not. All of the evidence, so far, is very weak (if it can be called evidence at all!). Still, nobody would suggest that Bisphenol A has much to recommend itself as a healthy addition to our diets. It seems prudent to try to limit our exposure to this compound when feasible, particularly among infants and pregnant women.
1. Pleskacova J, Hersmus R, Oosterhuis JW, Setyawati BA, Faradz SM, Cools M, Wolffenbuttel KP, Lebl J, Drop SL, Looijenga LH. Tumor Risk in Disorders of Sex Development. Sex Dev 4:259-269, 2010.
2. Skakkebaek NE, Rajpert-De Meyts E, Jorgensen N, Main KM, Leffers H, Andersson AM, Juul A, Jensen TK, Toppari J. Testicular cancer trends as 'whistle blowers' of testicular developmental problems in populations. Int J Androl 30:198-204, 2007.
3. Bouskine A, Nebout M, Brucker-Davis F, Benahmed M, Fenichel P. Low Doses of Bisphenol A Promote Human Seminoma Cell Proliferation by Activating PKA and PKG via a Membrane G-Protein-Coupled Estrogen Receptor. Environ Health Perspect 117:1053-1058, 2009.
This series of blogs has drawn heavily from the public use SEER data sets produced by the U.S. National Cancer Institute's Surveillance, Epidemiology and End Results project. In the next blog, I'll discuss how this data can be obtained and used by the science-minded public.
Jump to Tomorrow's blog
- © 2010 Jules Berman
key words: carcinogenesis, neoplasia, neoplasms, tumor development, tumour development, germ cell tumor, germ cell tumour, tumor epidemiology, increasing germ cell cancer rates, germ cell cancer, seminomas, seminomatous, non-seminomatous, non-germinomatous, embryonal carcinoma, choriocarcinoma, testis, testes, itgcn, intratubular germ cell neoplasm, plasticizers, endocrine disruptors
About my book, Precancer: The Beginning and the End of Cancer. Nearly every type of cancer passes through a precancer phase, during which it cannot metastasize or invade other tissues. While medicine is not always successful in treating or curing advanced stages of cancers, recent advances in our understanding of carcinogenesis have helped us to develop strategies to prevent, diagnose, and treat many cancers at the precancer stage. Research in this field is escalating rapidly as the evidence increasingly shows that the number of annual cancer deaths could be drastically reduced through the effective treatment and cure of precancer lesions. This book begins by explaining why it has been so difficult to cure cancers, followed by a review of precancer biology, with descriptions of the most common precancer lesions. The final chapters provide practical socio-political and medical goals for precancer treatment, including discussions of the economics and politics of treating precancers.

I urge you to read more about this important topic. Google Books has provided a generous preview of this book.
What can explain this increase?
There is one class of conditions that is overwhelmingly associated with the development of germ cell tumors of the testis: disorders of sex development of the testes.[1] Among the conditions within this general group are testicular dysgenesis, testicular feminization (insensitivity to androgens), and cryptorchidism. Disorders of sex development of the testis raise the incidence of intratubular germ cell neoplasia or of gonadoblastoma, both of which are testicular precancers.
As you might expect, along with the observed increase in testicular germ cell cancers in white males, there has been an observed increase in the incidence of disorders of sex development in the same population. [1,2] These disorders are characterized by a retardation in the maturation of primordial germ cells, along with an apparent mitotic over-stimulation of these same cells: leading to a proliferative, precancerous condition.
Though there is no proof at the moment, we might expect that males who develop testicular germ cell cancer who have clinically normal testes, may harbor small foci of [clinically unobserved] germ cell proliferative lesions.
What has caused the increased incidence of disorders of sex development in the testes? We don't know, but we have a candidate: the ubiquitous plasticizer and endocrine disruptor, Bisphenol A.
Bisphenol A is a synthetic estrogen used in the process of manufacturing plastics, and has been detected in the serum, milk, saliva, urine, and amniotic fluid of humans.[3] Because we get our daily dose of Bisphenol A from plastic bottles, one would expect that the levels of Bisphenol A in our blood would have increased steadily over the past several decades [coinciding with our increased dependence of plastic food and drink containers]. You might also expect that if Bisphenol A produced testicular cancers, you would see the largest increases in incidence among the wealthiest populations in the most industrialized nations [as we do].
Can we assume that Bisphenol A is causing the rise of incidence of testicular germ cell cancers? Absolutely not. All of the evidence, so far, is very weak (if it can be called evidence at all!). Still, nobody would suggest that Bisphenol A has much to recommend itself as a healthy addition to our diets. It seems prudent to try to limit our exposure to this compound when feasible, particularly among infants and pregnant women.
1. Pleskacova J, Hersmus R, Oosterhuis JW, Setyawati BA, Faradz SM, Cools M, Wolffenbuttel KP, Lebl J, Drop SL, Looijenga LH. Tumor Risk in Disorders of Sex Development. Sex Dev 4:259-269, 2010.
2. Skakkebaek NE, Rajpert-De Meyts E, Jorgensen N, Main KM, Leffers H, Andersson AM, Juul A, Jensen TK, Toppari J. Testicular cancer trends as 'whistle blowers' of testicular developmental problems in populations. Int J Androl 30:198-204, 2007.
3. Bouskine A, Nebout M, Brucker-Davis F, Benahmed M, Fenichel P. Low Doses of Bisphenol A Promote Human Seminoma Cell Proliferation by Activating PKA and PKG via a Membrane G-Protein-Coupled Estrogen Receptor. Environ Health Perspect 117:1053-1058, 2009.
This series of blogs has drawn heavily from the public use SEER data sets produced by the U.S. National Cancer Institute's Surveillance, Epidemiology and End Results project. In the next blog, I'll discuss how this data can be obtained and used by the science-minded public.
Jump to Tomorrow's blog
- © 2010 Jules Berman
key words: carcinogenesis, neoplasia, neoplasms, tumor development, tumour development, germ cell tumor, germ cell tumour, tumor epidemiology, increasing germ cell cancer rates, germ cell cancer, seminomas, seminomatous, non-seminomatous, non-germinomatous, embryonal carcinoma, choriocarcinoma, testis, testes, itgcn, intratubular germ cell neoplasm, plasticizers, endocrine disruptors
About my book, Precancer: The Beginning and the End of Cancer. Nearly every type of cancer passes through a precancer phase, during which it cannot metastasize or invade other tissues. While medicine is not always successful in treating or curing advanced stages of cancers, recent advances in our understanding of carcinogenesis have helped us to develop strategies to prevent, diagnose, and treat many cancers at the precancer stage. Research in this field is escalating rapidly as the evidence increasingly shows that the number of annual cancer deaths could be drastically reduced through the effective treatment and cure of precancer lesions. This book begins by explaining why it has been so difficult to cure cancers, followed by a review of precancer biology, with descriptions of the most common precancer lesions. The final chapters provide practical socio-political and medical goals for precancer treatment, including discussions of the economics and politics of treating precancers.
I urge you to read more about this important topic. Google Books has provided a generous preview of this book.
Tuesday, October 5, 2010
Explaining the germ cell cancer rates
In yesterday's blog we explained how the precancer of testicular germ cell tumors, intratubular germ cell neoplasia, gives rise to seminomas (differentiated germinomatous lineage) and non-seminomas (tumors of pluripotent progenitor cells that are not of germ cell lineage).
In the first blog of this series on germ cell tumors , we noted that the increase in occurrences of seminomas has outpaced the occurrences of the nonseminomatous germ cell tumors.
Here is a graph, produced from the SEER public use data sets, of the crude occurrences of seminoma and non-seminoma testicular germ cell tumors, in white males, since 1973.

The light blue bars are the seminomas, and the maroon bars are the non-seminomatous germ cell tumors of the testes. Since 1973, the seminomas increased from a number much lower than the occurrences of the non-seminomatous germ cell tumors; exceeding them in 1977. Since 1977, the crude occurrences of seminomas has greatly outpaced the occurrences of the non-seminomatous germ cell tumors of testes in white males.
Why? If both types of tumors are coming from the same precancer, why are their trends of occurrence non-parallel?
Well, there are several possible answers. It is possible that some external influence has modified the step in the progression of precancer to cancer, to favor the occurrence of seminomas.
However, it is also possible that their increases in occurrence are indeed parallel, and we're just not seeing it in our graph. Bray et al have looked at the incidence of testicular seminoma and non-seminoma germ cell tumors, by cohort (i.e., year of birth), not by year of occurrence.[1]
Bray F, Richiardi L, Ekbom A, Forman D,Pukkala E, Cuninkova M, Moller H. Do Testicular Seminoma and Nonseminoma Share the Same Etiology? Evidence from an Age-Period-Cohort Analysis of Incidence Trends in Eight European Countries. Cancer Epidemiol Biomarkers Prev 15:652–658, 2006.
When the comparisons are based on cohort (comparing incidence for people born the same year), most of the differences vanish [between the incidence of seminomas and non-seminomatous germ cell tumors].
When do we see a birth corhort effect on tumor incidence? For cancers, a cohort effect is best observed when individuals born in one year are exposed (as a population group) to a causal agent that is different from the exposure of individuals born in other years. The cancers that result may occur at many different ages, thus erasing the cohort effect when the data is stratified by year of occurrence (as we had done the graph above). Only when you look at the birth cohort will you find a trend that may relate to a carcinogenic exposure.
OK. The birth cohort data reported by Bray et al would seem to indicate that some generational effect is acting on succeeding cohorts to produce a shared increase in the incidence of all testicular germ cell cancers. Furthermore, whatever is causing the generational effect is likely to be of short duration or differ significantly from year to year. Why is that? If the exposure of a carcinogen were of long duration or were the same from year to year, then every cohort would be exposed similarly, and there would be no birth-year specific effect.
So, now the mystery is: What are the conditions and carcinogens that might cause testicular germ cell tumors, which have changed, year-by-year, to produce the observed rise in these cancers in white males? This will be the topic of the next blog.
Jump to Tomorrow's Blog
- © 2010 Jules Berman
key words: carcinogenesis, neoplasia, neoplasms, tumor development, tumour development, germ cell tumor, germ cell tumour, tumor epidemiology, increasing germ cell cancer rates, germ cell cancer, seminomas, seminomatous, non-seminomatous, non-germinomatous, embryonal carcinoma, choriocarcinoma, testis, testes, itgcn, intratubular germ cell neoplasm
Science is not a collection of facts. Science is what facts teach us; what we can learn about our universe, and ourselves, by deductive thinking. From observations of the night sky, made without the aid of telescopes, we can deduce that the universe is expanding, that the universe is not infinitely old, and why black holes exist. Without resorting to experimentation or mathematical analysis, we can deduce that gravity is a curvature in space-time, that the particles that compose light have no mass, that there is a theoretical limit to the number of different elements in the universe, and that the earth is billions of years old. Likewise, simple observations on animals tell us much about the migration of continents, the evolutionary relationships among classes of animals, why the nuclei of cells contain our genetic material, why certain animals are long-lived, why the gestation period of humans is 9 months, and why some diseases are rare and other diseases are common. In “Armchair Science”, the reader is confronted with 129 scientific mysteries, in cosmology, particle physics, chemistry, biology, and medicine. Beginning with simple observations, step-by-step analyses guide the reader toward solutions that are sometimes startling, and always entertaining. “Armchair Science” is written for general readers who are curious about science, and who want to sharpen their deductive skills.
In the first blog of this series on germ cell tumors , we noted that the increase in occurrences of seminomas has outpaced the occurrences of the nonseminomatous germ cell tumors.
Here is a graph, produced from the SEER public use data sets, of the crude occurrences of seminoma and non-seminoma testicular germ cell tumors, in white males, since 1973.

The light blue bars are the seminomas, and the maroon bars are the non-seminomatous germ cell tumors of the testes. Since 1973, the seminomas increased from a number much lower than the occurrences of the non-seminomatous germ cell tumors; exceeding them in 1977. Since 1977, the crude occurrences of seminomas has greatly outpaced the occurrences of the non-seminomatous germ cell tumors of testes in white males.
Why? If both types of tumors are coming from the same precancer, why are their trends of occurrence non-parallel?
Well, there are several possible answers. It is possible that some external influence has modified the step in the progression of precancer to cancer, to favor the occurrence of seminomas.
However, it is also possible that their increases in occurrence are indeed parallel, and we're just not seeing it in our graph. Bray et al have looked at the incidence of testicular seminoma and non-seminoma germ cell tumors, by cohort (i.e., year of birth), not by year of occurrence.[1]
Bray F, Richiardi L, Ekbom A, Forman D,Pukkala E, Cuninkova M, Moller H. Do Testicular Seminoma and Nonseminoma Share the Same Etiology? Evidence from an Age-Period-Cohort Analysis of Incidence Trends in Eight European Countries. Cancer Epidemiol Biomarkers Prev 15:652–658, 2006.
When the comparisons are based on cohort (comparing incidence for people born the same year), most of the differences vanish [between the incidence of seminomas and non-seminomatous germ cell tumors].
When do we see a birth corhort effect on tumor incidence? For cancers, a cohort effect is best observed when individuals born in one year are exposed (as a population group) to a causal agent that is different from the exposure of individuals born in other years. The cancers that result may occur at many different ages, thus erasing the cohort effect when the data is stratified by year of occurrence (as we had done the graph above). Only when you look at the birth cohort will you find a trend that may relate to a carcinogenic exposure.
OK. The birth cohort data reported by Bray et al would seem to indicate that some generational effect is acting on succeeding cohorts to produce a shared increase in the incidence of all testicular germ cell cancers. Furthermore, whatever is causing the generational effect is likely to be of short duration or differ significantly from year to year. Why is that? If the exposure of a carcinogen were of long duration or were the same from year to year, then every cohort would be exposed similarly, and there would be no birth-year specific effect.
So, now the mystery is: What are the conditions and carcinogens that might cause testicular germ cell tumors, which have changed, year-by-year, to produce the observed rise in these cancers in white males? This will be the topic of the next blog.
Jump to Tomorrow's Blog
- © 2010 Jules Berman
key words: carcinogenesis, neoplasia, neoplasms, tumor development, tumour development, germ cell tumor, germ cell tumour, tumor epidemiology, increasing germ cell cancer rates, germ cell cancer, seminomas, seminomatous, non-seminomatous, non-germinomatous, embryonal carcinoma, choriocarcinoma, testis, testes, itgcn, intratubular germ cell neoplasm
Science is not a collection of facts. Science is what facts teach us; what we can learn about our universe, and ourselves, by deductive thinking. From observations of the night sky, made without the aid of telescopes, we can deduce that the universe is expanding, that the universe is not infinitely old, and why black holes exist. Without resorting to experimentation or mathematical analysis, we can deduce that gravity is a curvature in space-time, that the particles that compose light have no mass, that there is a theoretical limit to the number of different elements in the universe, and that the earth is billions of years old. Likewise, simple observations on animals tell us much about the migration of continents, the evolutionary relationships among classes of animals, why the nuclei of cells contain our genetic material, why certain animals are long-lived, why the gestation period of humans is 9 months, and why some diseases are rare and other diseases are common. In “Armchair Science”, the reader is confronted with 129 scientific mysteries, in cosmology, particle physics, chemistry, biology, and medicine. Beginning with simple observations, step-by-step analyses guide the reader toward solutions that are sometimes startling, and always entertaining. “Armchair Science” is written for general readers who are curious about science, and who want to sharpen their deductive skills.
Sunday, October 3, 2010
Germ cell precancers and epigenetic erasure
In yesterday's blog , we left off with a question: "How it is possible for intratubular germ cell neoplasia to be the precursor for both germinomatous germ cell cancers (i.e., seminoma) and non-germinomatous germ cell cancers (e.g. embryonal carcinoma, choriocarcinoma)?
The key is epigenetic erasure, a phenomenon unique to germ cells.
As an organism develops, cells specialize into about 200 differentiated cell types. All these different types of cells have the same genetic sequence (genome). Cell types are distingued, one from the other, by epigenetic modifications. Epigenetic modifications to genes involve base methylation, conformational changes in chromosomes, protein modifications... anything other than changes in DNA sequence.
Germ cells, like all other differentiated cells, have epigenetic modifications. The unique thing about germ cells is that they must undergo epigenetic erasure prior to the production of gametes; otherwise the gametes would be imprinted with the epigenetic modifications characteristic of the parent organism and would not be capable of recombining during fertilization to produce a fully de-differentiated, totipotent product.[1]
The cells of intratubular germ cell neoplasia (the precancer of most male germ cell tumors) and of seminomas, are all characterized by DNA hypomethylation; not so for the cells of non-germinomatous germ cell tumors.[2,3] DNA Hypomethylation is seen in epigenomic erasure [of germ cells].
"Erased" germ cells are capable of developing into totipotent embryonic cells.[4] It would seem that a plausible mechanism for the development of non-germinomatous germ cell cancers from a germ cell precursor (intratubular germ cell neoplasia, itgcn) is that the "erased" itgcn cells, during cancer development, transform into totipotent cells, capable of differentiating into cells from any embryonic layer (e.g., embryonal carcinoma), or into extra-embryonic tissue (e.g., choriocarcinoma).
This explains why the itgcn, the germ cell precancer, can give rise to both germinomatous (erased) and non-germinomatous (epigenetic-modified) cancers.
There is only one mystery left to solve (the original mystery that we started with, about 4 blog entries back ). If germinomatous and non-germinomatous germ cell cancers both arise from the same precursor, why is there a much greater increase in the rate of occurrence of seminomas compared with the rate of occurrence of non-germinomatous cancers, since 1973?
1. Allegrucci C, Thurston A, Lucas E, Young L. Epigenetics and the germline. Reproduction 129:137-149, 2005.
2. Netto GJ et al.Global DNA hypomethylation in intratubular germ cell neoplasia and seminoma, but not in nonseminomatous male germ cell tumors. Modern Pathology 21: 1337-1344, 2008.
3. Lind GE, Skotheim RI, Lothe RA. The epigenome of testicular germ cell tumors. APMIS (Acta Pathologica, Microbiologica et Immunologica Scandinavica) 115:1147-1160, 2007.
4. Turnpenny L. Derivation of human embryonic germ cells: an alternative source of pluripotent stem cells. Stem Cells 21:598-609, 2003.
Jump to Tomorrow's Blog
- © 2010 Jules Berman
key words: carcinogenesis, neoplasia, neoplasms, tumor development, tumour development, germ cell tumor, germ cell tumour, tumor epidemiology, increasing germ cell cancer rates, germ cell cancer, seminomas, seminomatous, non-seminomatous, non-germinomatous, embryonal carcinoma, choriocarcinoma, testis, testes, itgcn, intratubular germ cell neoplasm
In June, 2014, my book, entitled Rare Diseases and Orphan Drugs: Keys to Understanding and Treating the Common Diseases was published by Elsevier. The book builds the argument that our best chance of curing the common diseases will come from studying and curing the rare diseases.

I urge you to read more about my book. There's a generous preview of the book at the Google Books site. If you like the book, please request your librarian to purchase a copy of this book for your library or reading room.
The key is epigenetic erasure, a phenomenon unique to germ cells.
As an organism develops, cells specialize into about 200 differentiated cell types. All these different types of cells have the same genetic sequence (genome). Cell types are distingued, one from the other, by epigenetic modifications. Epigenetic modifications to genes involve base methylation, conformational changes in chromosomes, protein modifications... anything other than changes in DNA sequence.
Germ cells, like all other differentiated cells, have epigenetic modifications. The unique thing about germ cells is that they must undergo epigenetic erasure prior to the production of gametes; otherwise the gametes would be imprinted with the epigenetic modifications characteristic of the parent organism and would not be capable of recombining during fertilization to produce a fully de-differentiated, totipotent product.[1]
The cells of intratubular germ cell neoplasia (the precancer of most male germ cell tumors) and of seminomas, are all characterized by DNA hypomethylation; not so for the cells of non-germinomatous germ cell tumors.[2,3] DNA Hypomethylation is seen in epigenomic erasure [of germ cells].
"Erased" germ cells are capable of developing into totipotent embryonic cells.[4] It would seem that a plausible mechanism for the development of non-germinomatous germ cell cancers from a germ cell precursor (intratubular germ cell neoplasia, itgcn) is that the "erased" itgcn cells, during cancer development, transform into totipotent cells, capable of differentiating into cells from any embryonic layer (e.g., embryonal carcinoma), or into extra-embryonic tissue (e.g., choriocarcinoma).
This explains why the itgcn, the germ cell precancer, can give rise to both germinomatous (erased) and non-germinomatous (epigenetic-modified) cancers.
There is only one mystery left to solve (the original mystery that we started with, about 4 blog entries back ). If germinomatous and non-germinomatous germ cell cancers both arise from the same precursor, why is there a much greater increase in the rate of occurrence of seminomas compared with the rate of occurrence of non-germinomatous cancers, since 1973?
1. Allegrucci C, Thurston A, Lucas E, Young L. Epigenetics and the germline. Reproduction 129:137-149, 2005.
2. Netto GJ et al.Global DNA hypomethylation in intratubular germ cell neoplasia and seminoma, but not in nonseminomatous male germ cell tumors. Modern Pathology 21: 1337-1344, 2008.
3. Lind GE, Skotheim RI, Lothe RA. The epigenome of testicular germ cell tumors. APMIS (Acta Pathologica, Microbiologica et Immunologica Scandinavica) 115:1147-1160, 2007.
4. Turnpenny L. Derivation of human embryonic germ cells: an alternative source of pluripotent stem cells. Stem Cells 21:598-609, 2003.
Jump to Tomorrow's Blog
- © 2010 Jules Berman
key words: carcinogenesis, neoplasia, neoplasms, tumor development, tumour development, germ cell tumor, germ cell tumour, tumor epidemiology, increasing germ cell cancer rates, germ cell cancer, seminomas, seminomatous, non-seminomatous, non-germinomatous, embryonal carcinoma, choriocarcinoma, testis, testes, itgcn, intratubular germ cell neoplasm
In June, 2014, my book, entitled Rare Diseases and Orphan Drugs: Keys to Understanding and Treating the Common Diseases was published by Elsevier. The book builds the argument that our best chance of curing the common diseases will come from studying and curing the rare diseases.
I urge you to read more about my book. There's a generous preview of the book at the Google Books site. If you like the book, please request your librarian to purchase a copy of this book for your library or reading room.
Germ cell tumor common precancer: itgcn
In yesterday's blog , we discussed the terminology problem with the germ cell tumors. Basically, if you have a sub-class of germ cell tumors that are called "non-germinomatous germ cell tumors," isn't that a contradiction in terms? Isn't it like saying that dehydrated water is a subclass of water?
The answer is simple: the classic germ cell tumor of the testes (seminoma), as well as most of the malignant non-germinomatous germ cell tumors of the testes, arise from the same precancer: intratubular germ cell neoplasia (itgcn). Because itgcn is composed of dysplastic (early neoplastic) germ cells, both the germinomatous and non-germinomatous tumors have a germ cell origin.
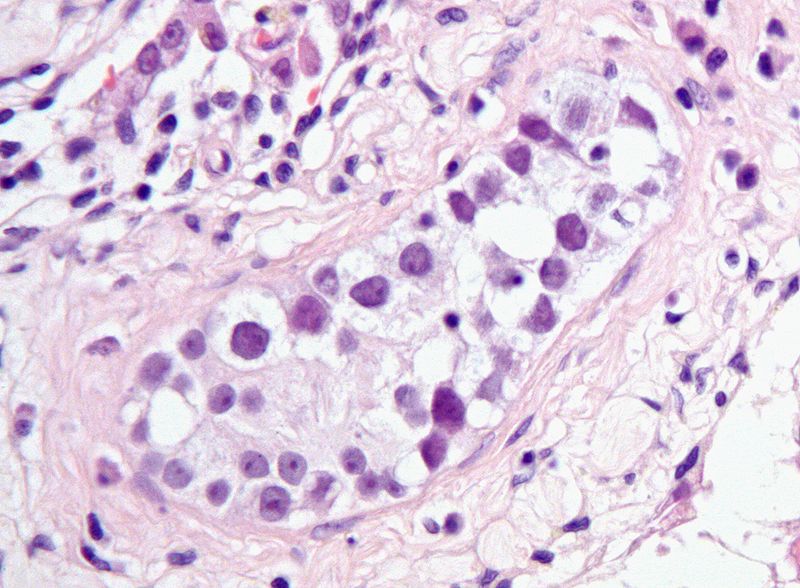
You can easily appreciate the morphologic similarity between itgcn and seminoma by looking at a histologic preparation of each.

Image of Intratubular Germ Cell neoplasia
Distributed by Wikimedia
under a Creative Commons License
The germ cell precancer, itgcn, is a collection of atypical gonocytic cells lining seminiferous tubules in the testis.

Image of Seminoma
Distributed by Wikimedia
under a GNU License
Seminoma cells closely resemble the cells of itgcn, from which they derive (with the rare exception of the so-called spermatocytic seminoma, which behaves unlike the other types of seminomas).
The same precancer (itgcn) precedes the development of most of the invasive non-germinomatous germ cell tumors of the testis.
So, the terminologic mystery is solved. The germinomatous and the non-germinomatous germ cell tumors are classified together because most of them are derived from neoplastic intratubular germ cells (i.e., intratubular germ cell neoplasia).
But solving the terminologic mystery does not help us understand the biology of what's happening. Why does itgcn give rise to tumors of germ cells (e.g., seminomas) and to tumors of primimitive non-germ cells (e.g., embryonal carcinoma, choriocarcinoma)? How can a tumor be derived from cells that have a committed lineage (i.e., sperm cells in the case of males) that is completely unrelated to the lineages found in the tumor?
There's an answer. It has a lot to do with a phenomenon unique to germ cells called epigenomic erasure. This will be the topic of the next blog in our series on germ cell tumors.
Jump to Tomorrow's Blog
- © 2010 Jules Berman
key words: carcinogenesis, neoplasia, neoplasms, tumor development, tumour development, germ cell tumor, germ cell tumour, tumor epidemiology, increasing germ cell cancer rates, germ cell cancer, seminomas, seminomatous, non-seminomatous, non-germinomatous, embryonal carcinoma, choriocarcinoma, testis, testes, itgcn, intratubular germ cell neoplasm
In June, 2014, my book, entitled Rare Diseases and Orphan Drugs: Keys to Understanding and Treating the Common Diseases was published by Elsevier. The book builds the argument that our best chance of curing the common diseases will come from studying and curing the rare diseases.
I urge you to read more about my book. There's a generous preview of the book at the Google Books site. If you like the book, please request your librarian to purchase a copy of this book for your library or reading room.
The answer is simple: the classic germ cell tumor of the testes (seminoma), as well as most of the malignant non-germinomatous germ cell tumors of the testes, arise from the same precancer: intratubular germ cell neoplasia (itgcn). Because itgcn is composed of dysplastic (early neoplastic) germ cells, both the germinomatous and non-germinomatous tumors have a germ cell origin.
You can easily appreciate the morphologic similarity between itgcn and seminoma by looking at a histologic preparation of each.
{kind=link}
Distributed by Wikimedia
under a Creative Commons License
The germ cell precancer, itgcn, is a collection of atypical gonocytic cells lining seminiferous tubules in the testis.

_nodal_metastasis.jpg){kind=link}
Distributed by Wikimedia
under a GNU License
Seminoma cells closely resemble the cells of itgcn, from which they derive (with the rare exception of the so-called spermatocytic seminoma, which behaves unlike the other types of seminomas).
The same precancer (itgcn) precedes the development of most of the invasive non-germinomatous germ cell tumors of the testis.
So, the terminologic mystery is solved. The germinomatous and the non-germinomatous germ cell tumors are classified together because most of them are derived from neoplastic intratubular germ cells (i.e., intratubular germ cell neoplasia).
But solving the terminologic mystery does not help us understand the biology of what's happening. Why does itgcn give rise to tumors of germ cells (e.g., seminomas) and to tumors of primimitive non-germ cells (e.g., embryonal carcinoma, choriocarcinoma)? How can a tumor be derived from cells that have a committed lineage (i.e., sperm cells in the case of males) that is completely unrelated to the lineages found in the tumor?
There's an answer. It has a lot to do with a phenomenon unique to germ cells called epigenomic erasure. This will be the topic of the next blog in our series on germ cell tumors.
Jump to Tomorrow's Blog
- © 2010 Jules Berman
key words: carcinogenesis, neoplasia, neoplasms, tumor development, tumour development, germ cell tumor, germ cell tumour, tumor epidemiology, increasing germ cell cancer rates, germ cell cancer, seminomas, seminomatous, non-seminomatous, non-germinomatous, embryonal carcinoma, choriocarcinoma, testis, testes, itgcn, intratubular germ cell neoplasm
In June, 2014, my book, entitled Rare Diseases and Orphan Drugs: Keys to Understanding and Treating the Common Diseases was published by Elsevier. The book builds the argument that our best chance of curing the common diseases will come from studying and curing the rare diseases.
I urge you to read more about my book. There's a generous preview of the book at the Google Books site. If you like the book, please request your librarian to purchase a copy of this book for your library or reading room.
Saturday, October 2, 2010
Germ cell tumors: definition problems
OK, getting back to the prior post on germ cell tumors, we found that the rate of occurrence of seminomatous germ cell tumors of the testes has been greatly increasing, in the white male population, since (at least) 1973. During the same period, the rate of occurrence of the other type of germ cell tumors (non-seminomatous) has hardly increased at all, for white men.
Why has the rate of occurrence of seminomas increased since 1973, in the white male population? Also, if seminomatous and non-seminomatous germ cell tumors are just morphologic variants of the same basic tumor (i.e., germ cell tumor), why wouldn't they both increase to the same extent?
Perhaps some of the problem relates to the definition of these two tumors.
Seminomas are tumors of gonocytes, a differentiated cell committed to producing gametes (sperm in males, eggs in females), or a committed progenitor cell of gamete-producing cells (i.e., an ancestral cell of a gamete-producing cell). Since seminomas are considered the neoplastic equivalent of gonocytes, there seems to be little leeway in their classification: they must be included among the germ cell tumors.
But what about the other type of germ cell tumors. This other type is known by two different names that tell us a lot about the ambivalent nature of the tumor:
From wikipedia:
"The nongerminomatous or nonseminomatous germ cell tumors (NGGCT, NSGCT) include all other germ cell tumors, pure and mixed."
How can a germ cell tumor be non-germinomatous? Wouldn't the adjective "non-germinomatous" pretty much tell you that the tumor can't be a germ cell tumor?
It reminds me of one of my favorite limericks.
As I was sitting in my chair,
I sensed the bottom was not there.
Nor legs, nor back,
But I just sat,
Ignoring little things like that.
- Anonymous
Well, what are the non-germinomatous germ cell tumors? These are tumors that usually arise in the gonads and are composed of primitive pluripotent cells. We can find pure or mixed populations of embryonal carcinoma, teratomatous tissue, and choriocarcinoma in the non-germinomatous germ cell tumors. These are the same cells that are found in the very earliest embryo and placenta. But these primitive cell types are not gonocytes (i.e., they are not differentiated cells committed to producing sperm or eggs). These tumors are composed of primitive non-germ cells.
So why are the primitive non-germ cell tumors included among the germ cell tumors?
The answer to this question comes from our understanding of the common precancer of most of the seminomatous and non-seminomatous germ cell tumors: intratubular germ cell neoplasia.
In the next several blogs, we'll discuss germ cell precancer, and we'll explain the unifying concept of germ cell neoplasia. We'll also see how a study of precancers is crucial to our understanding of neoplasia, in general.
Jump to Tomorrow's Blog
- © 2010 Jules Berman
key words: carcinogenesis, neoplasia, neoplasms, tumor development, tumour development, germ cell tumor, germ cell tumour, tumor epidemiology, increasing germ cell cancer rates, germ cell cancer, seminomas, seminomatous
In June, 2014, my book, entitled Rare Diseases and Orphan Drugs: Keys to Understanding and Treating the Common Diseases was published by Elsevier. The book builds the argument that our best chance of curing the common diseases will come from studying and curing the rare diseases.
I urge you to read more about my book. There's a generous preview of the book at the Google Books site. If you like the book, please request your librarian to purchase a copy of this book for your library or reading room.
Why has the rate of occurrence of seminomas increased since 1973, in the white male population? Also, if seminomatous and non-seminomatous germ cell tumors are just morphologic variants of the same basic tumor (i.e., germ cell tumor), why wouldn't they both increase to the same extent?
Perhaps some of the problem relates to the definition of these two tumors.
Seminomas are tumors of gonocytes, a differentiated cell committed to producing gametes (sperm in males, eggs in females), or a committed progenitor cell of gamete-producing cells (i.e., an ancestral cell of a gamete-producing cell). Since seminomas are considered the neoplastic equivalent of gonocytes, there seems to be little leeway in their classification: they must be included among the germ cell tumors.
But what about the other type of germ cell tumors. This other type is known by two different names that tell us a lot about the ambivalent nature of the tumor:
From wikipedia:
"The nongerminomatous or nonseminomatous germ cell tumors (NGGCT, NSGCT) include all other germ cell tumors, pure and mixed."
How can a germ cell tumor be non-germinomatous? Wouldn't the adjective "non-germinomatous" pretty much tell you that the tumor can't be a germ cell tumor?
It reminds me of one of my favorite limericks.
As I was sitting in my chair,
I sensed the bottom was not there.
Nor legs, nor back,
But I just sat,
Ignoring little things like that.
- Anonymous
Well, what are the non-germinomatous germ cell tumors? These are tumors that usually arise in the gonads and are composed of primitive pluripotent cells. We can find pure or mixed populations of embryonal carcinoma, teratomatous tissue, and choriocarcinoma in the non-germinomatous germ cell tumors. These are the same cells that are found in the very earliest embryo and placenta. But these primitive cell types are not gonocytes (i.e., they are not differentiated cells committed to producing sperm or eggs). These tumors are composed of primitive non-germ cells.
So why are the primitive non-germ cell tumors included among the germ cell tumors?
The answer to this question comes from our understanding of the common precancer of most of the seminomatous and non-seminomatous germ cell tumors: intratubular germ cell neoplasia.
In the next several blogs, we'll discuss germ cell precancer, and we'll explain the unifying concept of germ cell neoplasia. We'll also see how a study of precancers is crucial to our understanding of neoplasia, in general.
Jump to Tomorrow's Blog
- © 2010 Jules Berman
key words: carcinogenesis, neoplasia, neoplasms, tumor development, tumour development, germ cell tumor, germ cell tumour, tumor epidemiology, increasing germ cell cancer rates, germ cell cancer, seminomas, seminomatous
In June, 2014, my book, entitled Rare Diseases and Orphan Drugs: Keys to Understanding and Treating the Common Diseases was published by Elsevier. The book builds the argument that our best chance of curing the common diseases will come from studying and curing the rare diseases.
I urge you to read more about my book. There's a generous preview of the book at the Google Books site. If you like the book, please request your librarian to purchase a copy of this book for your library or reading room.
Friday, October 1, 2010
Povray script for book cover
Currently, I'm writing a series of blogs on germ cell tumors. But I took a break today to prepare a web page that provides the PovRay script for the cover image of my new book, Methods in Medical Informatics, Fundamental of Healthcare Programming in Perl, Python, and Ruby.

The PovRay script and a high-resoluion version of the image used in the book cover, are available at:
http://www.julesberman.info/book/coverhow.htm
I'll resume the germ cell tumor series soon.
- Jules Berman
Science is not a collection of facts. Science is what facts teach us; what we can learn about our universe, and ourselves, by deductive thinking. From observations of the night sky, made without the aid of telescopes, we can deduce that the universe is expanding, that the universe is not infinitely old, and why black holes exist. Without resorting to experimentation or mathematical analysis, we can deduce that gravity is a curvature in space-time, that the particles that compose light have no mass, that there is a theoretical limit to the number of different elements in the universe, and that the earth is billions of years old. Likewise, simple observations on animals tell us much about the migration of continents, the evolutionary relationships among classes of animals, why the nuclei of cells contain our genetic material, why certain animals are long-lived, why the gestation period of humans is 9 months, and why some diseases are rare and other diseases are common. In “Armchair Science”, the reader is confronted with 129 scientific mysteries, in cosmology, particle physics, chemistry, biology, and medicine. Beginning with simple observations, step-by-step analyses guide the reader toward solutions that are sometimes startling, and always entertaining. “Armchair Science” is written for general readers who are curious about science, and who want to sharpen their deductive skills.

The PovRay script and a high-resoluion version of the image used in the book cover, are available at:
http://www.julesberman.info/book/coverhow.htm
I'll resume the germ cell tumor series soon.
- Jules Berman
Science is not a collection of facts. Science is what facts teach us; what we can learn about our universe, and ourselves, by deductive thinking. From observations of the night sky, made without the aid of telescopes, we can deduce that the universe is expanding, that the universe is not infinitely old, and why black holes exist. Without resorting to experimentation or mathematical analysis, we can deduce that gravity is a curvature in space-time, that the particles that compose light have no mass, that there is a theoretical limit to the number of different elements in the universe, and that the earth is billions of years old. Likewise, simple observations on animals tell us much about the migration of continents, the evolutionary relationships among classes of animals, why the nuclei of cells contain our genetic material, why certain animals are long-lived, why the gestation period of humans is 9 months, and why some diseases are rare and other diseases are common. In “Armchair Science”, the reader is confronted with 129 scientific mysteries, in cosmology, particle physics, chemistry, biology, and medicine. Beginning with simple observations, step-by-step analyses guide the reader toward solutions that are sometimes startling, and always entertaining. “Armchair Science” is written for general readers who are curious about science, and who want to sharpen their deductive skills.
Subscribe to:
Posts (Atom)